
Federation University Australia is committed to quality assurance and continuous improvement across its federated network of campuses and partner-provider institutions. The Quality Framework describes the approach to quality assurance by embedding principles of good practice in quality management in accordance with the statutory quality standards of its regulatory bodies through a system of mature quality assurance processes, compliance auditing and the capture and implementation of continuous improvement.
The University is bound by regulatory and legislative frameworks that guide our educational practice, both federal and state based. This Quality Framework outlines the University’s approach to compliance with the requirements stipulated within these regulatory and legislative requirements for all University courses delivered to domestic and international students and requirements for partner providers delivering Federation University courses.
The Regulatory Point of Contact enables the University to consolidate and monitor all queries to the University’s regulatory bodies: Australian Skills Quality Authority ASQA, the Tertiary Education Quality and Standards Agency (TEQSA), the Victorian Registration and Qualifications Authority (VRQA) and the Department of Jobs, Skills, Industry and Regions (DJSIR) to one contact point within the University.
The University will provide a quality tertiary education experience that inspires its students to succeed, serves its regions and communities, and is international in its outlook and impact.
This document applies to all organisational units, campuses, staff and functions of the University, inclusive of the entire University community including students and partners of the University located locally, interstate and overseas, and is supported by the University's Strategic Plan.
This procedure does not encompass the regulations or requirements of licensing or accrediting bodies.
- Federation University Australia Act 2010
- Higher Education Standards Framework (HESF 2021)
- Standards for Registered Training Organisations RTO 2025
- National Code of Practice for Providers of Education and Training to Overseas Students 2018 ( National Code 2018)
- Education Services for Overseas Students Act 2000 (ESOS)
- ESOS Regulations 2019
- ESOS (Registration Charges) Act 1997
- ESOS (TPS Levies) Act 2012
The statutory requirements of the following regulatory bodies are adhered to:
- Australia Skills Quality Authority ASQA
- Victorian Registration Qualifications Authority (VRQA)
- Tertiary Education Quality and Standards Agency (TEQSA)
- Department Jobs, Skills, Industry and Regions; VET Funding Contract
| Term | Definition |
| Academic Board |
The principal academic body of the University whose purpose is twofold: firstly, to provide academic oversight of prescribed academic courses and units of study of higher education and VET in the University; and secondly to provide advice to Council on the conduct and content of those courses and units. Specific responsibilities in the context of this Quality Framework are:
Academic Board is supported in these duties by its Standing Committees. Please refer to http://federation.edu.au/staff/governance/academic-board/standing-committees for further detail on these committees. |
| Act | Federation University Australia Act 2010 provides the legislative framework that the University is required to operate under. |
| Benchmarking | The process of measuring and monitoring outcomes against predetermined (usually best practice) standards. |
| Continuous improvement | The ongoing process of change for the purpose of improvement to practices and processes. |
| Council | The Council is the governing authority of the University and is responsible for the direction and superintendence of the University. |
| Institutes and Schools | Federation University Australia has a number of Academic Organisational Units - click here for details. |
| Governance | The processes by which the University is controlled and held to account. It encompasses authority, accountability, stewardship, leadership, direct and control exercised in the organisation (Standards Australia AS 8000-2003/Amdt 1-2004). |
| Onshore Students | A person holding an Australian student visa and is defined as an 'Overseas Student' in the ESOS Act. |
| Partner-provider organisation | Educational institution providing courses and units of the University through an approved Education Agreement. |
| Policy | A formal statement of principle that regulates University operations |
| Procedure | Describes the operational processes/steps to be adhered to in order to maintain effective adherence to the prescribed principles outlined in the associated policy. |
| Quality assurance | The program of activities to ensure products and services are of the desired quality. |
| Quality framework | The system in which activities used to carry out Quality Control, Quality Assurance and Continuous Improvement are completed at the University. |
| Quality cycle | The cyclic process of planning, quality improvement, quality control, quality and data reporting and quality improvement, including but not limited to benchmarking, audits, reviews and program, course and units review. |
| Regulation | Made by Council under a University Statute to regulate interpretation and implementation of the Statute. |
| Regulator Standards | The Higher Education Standards Framework (TEQSA) and the Australian Skills Quality Authority ASQA under the National Vocational Education and Training Regulator Act 2011, Victorian Registration and Qualifications Authority (VRQA). |
| Standing Committees | Permanent committees established under and reporting to Council -refer http://federation.edu.au/staff/governance/academic-board/standing-committees. |
| Statute | The subordinate legislations related to the governance of the internal affairs of the University under the Federation University Australia Act 2010 (as listed in Part 5 Section 29 of the Act). Statutes can only be made, amended, or revoked by Council and must be approved by the relevant State Minister with responsibility for tertiary education. A University Statute comes into operation on the day on which the Minister approves it (unless otherwise specified in the Statute). |
Federation University Australia is established under the Federation University Australia Act 2010. Under the Act, the decision making powers of the University lie with Council as its governing body, Academic Board and the Vice-Chancellor. The University is responsible to comply with the statutory requirements as listed under Legislative Context.
The University Quality Framework in conjunction with regulatory and legislative requirements at the University has two objectives:
- To comply with the Federation University Australia Act 2010 and the decision- making powers of the University that lie with Council as its governing body, Academic Board and the Vice-Chancellor complying with the statutory requirements as listed under Legislative Context
- To maintain University compliance with regulatory and legislative requirements to ensure continuing registration and certification as a Self-Accrediting Institution and as a Registered Training Organisation
|
UNIVERSITY GOVERNANCE Council and Standing Committees of Council | |
|
MANAGEMENT/OPERATIONS Vice-Chancellor Vice-Chancellor Senior Team (VCST) Operational Leadership (Executive Deans, Heads of Operational Areas, Directors) All employees Students and other members |
ACADEMIC GOVERNANCE Academic Board and Standing Committees of Academic Board |
This tripartite governance structure in which management and academic board contribute to academic decision-making, within the context of Council's overall responsibility and decisions ensures a clear distinction between governance and management responsibilities and clear separation between corporate and academic governance.
The University's quality framework is whole-of-institution, linking strategic principles and strategic directions with planning and best practice in quality management.
| University Principle | Demonstrated through the Quality Framework by: |
| Excellence |
|
| Relevance |
|
| Inclusive |
|
| Empowering |
|
| Innovative and agile |
|
The University, with the support of Quality Assurance Services actively plans for quality assurance of the University as well as seeking opportunities to enhance best practice through continuous improvement.
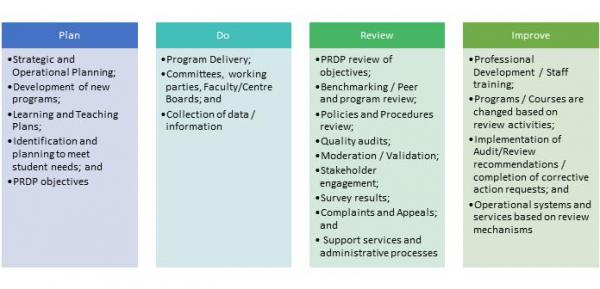
Federation University Australia has adopted the Continuous Improvement Cycle of Plan, Do, Review and Improve to drive the process for self-review, reflection, continuous improvement and accountability to assure internal and external accreditation, registration and relevant audits.
Federation University's quality approach is aligned to the relevant regulatory standards, the student lifecycle, and the University's Strategic objectives and outcomes. The University has documented policies and procedures that provide clear instruction on how the Quality Framework is implemented across the University and its Partner Provider teaching locations. Compliance with all regulatory frameworks, is a university-wide effort, commitment and responsibility.
| Activity | Responsibility | Steps | |
| 1. | Plan Internal Quality audit | Senior Manager, Quality Assurance Services |
The Internal Quality Audit schedule is developed and released quarterly, in consultation with relevant stakeholders taking into account:
|
| 2. | Conduct Audits. | Quality Assurance Services |
|
| 3. |
Report on Quality Audits |
Quality Services/ Auditee |
|
| 4. |
Review non-compliances and proposed rectifications |
Quality Services |
|
| 5 | Committee and Operational Area Quality Audits |
Operational Areas University Governance and Management Committees |
Audits are conducted and reported in line with the internal business process of the operational area or committee conducting the audit. |
The purpose of ESOS and HESF audits is to ensure that the University is compliant with the ESOS Act 2000, the National Code 2018 and the Higher Education Standards Framework (Threshold Standards) 2021. On and offshore partners who deliver University programs to international students will be audited for ESOS and/or HESF compliance.
| Activity | Responsibility | Steps | |
| 1. | Plan Partner Provider ESOS and HES Audit (On & Off Shore) and on-campus ESOS audits. | Senior Manager, Quality Assurance Services |
|
| 2. | Conduct Audit | Senior Manager, Quality Assurance Services or Quality Officer |
When conducting an ESOS / HESF audit, use the relevant audit template for guidance for areas of required compliance to be audited. The audit templates are:
Provide the template to the Partner Provider and / or Schools / Institutes to assist with their preparation. For the desktop audits, meet with University staff, review student management systems, review Partner Provider websites and request materials electronically. Where necessary due to responses in the self-assessment and / or result of a desktop audit a follow-up onsite audit will be conducted even if not listed in the audit schedule. The lead auditor is responsible for an Onsite Audit – Opening Meeting. Meet with the senior Partner Provider and / or School / Institute staff involved in the audit to ensure that they are clear about the processes and activities that will be undertaken by the auditing team. The following should be discussed at the Opening Meeting:
|
| 3. | Report on International and Partnerships Compliance Audits: | Senior Manager, Quality Assurance Services or Quality Officer |
Recording Information:
Audit Report Structure Upon completion of an audit, a report documenting the findings of the audit must be completed. For Partner Provider audits, clearly itemise findings under each area audited. At the end of each report, in the section titled “Summary of Audit Findings” include the compliant (C), non-compliant (NC) and Opportunities for Improvement (OFI). Append a Non-compliance Rectification request (NCR) to the report.
If the audited Partner Provider and / or School / Institute advise that they have rectified the non-compliances listed in the report, do not remove from report. The report reflects a point-in-time audit, an additional note can be added to advise that the non-compliance has been addressed. Evidence must be provided.
|
| 4. | Review International and Partnerships Compliance Audits: | Senior Manager, Quality Assurance Services or Quality Officer |
|
Internal Audits are an integral part of the University's Governance framework. The function provides the University Council and Audit and Risk Management Committee with independent and objective assurance that internal controls are operating as intended and that they are adequate to minimise risk and assist the University to achieve its strategic goals.
The Internal Audit function also assists the University to achieve sound managerial review of all of its operations to ensure that activities are being carried as effectively and efficiently as possible.
|
Activity
|
Responsibility | Steps | |
| 1 | Plan: Develop 3 - 4 year Strategic Internal Audit Plan and Annual Internal Audit Work Plan |
Director, Strategy Audit and Risk Management Committee |
|
| 2 | Conduct: Determine Internal audit scope and conduct audit |
Director, Strategy Audit and Risk Management Committee |
|
| 3 | Report: Draft Internal audit reports and submit for approval |
Director, Strategy Audit and Risk Committee |
|
| 4 | Review: Audit actions and regulatory compliance status briefings | Director, Strategy and Vice- Chancellor |
|
Council is required to review its operation and performance in accordance with the standing Council resolution CM5/05/08, Procedure for Assessment of Council Members Performance and Universities Australia ‘Voluntary Code of Best Practice for the Governance of Australian Universities’.
In accordance with the standing resolution, Council will undertake a formal assessment of the performance of Council and its Standing Committees on an annual basis and a comprehensive external review at least every five years.
| Activity | Responsibility | Steps | |
| 1. | Plan to conduct a review of Standing Committees of Council | Executive Officer – Council and Committees of Council |
Evaluation form for Assessment of Committee Performance is distributed annually in October to each Standing Committee. A complete listing of the Standing Committees of Council can be found on the Council web site at https://federation.edu.au/staff/governance/feduni-council/council-committees The criteria for the evaluation must align with each Committee’s Terms of Reference and responsibilities. |
| 2. | Standing Committee conduct review | Executive Officer – Council and Committees of Council | Once the Standing Committee has conducted its review, responses are collated, de-identified and summarised into a document which is then reviewed by the Committee. |
| 3. | Review tabled at Governance and Strategy Committee and Council for consideration | Executive Officer – Council and Committees of Council | The summarised review document from the Standing Committee is sent to the November meeting of Governance & Strategy Committee and then forwarded as soon as practicable thereafter to Council. |
| 4. | Results from the Standing Committee reviews are considered by the Council | Chancellor |
Results from the Standing Committee reviews are considered by the Chair of the Standing Committee and then forwarded to the Governance & Strategy Committee when conducting the annual Terms of Reference review for each standing committee. The Governance & Strategy Committee conducts annual reviews in February of the Terms of Reference of all Council standing committees to ensure currency and relevance. |
| Activity | Responsibility | Steps | |
| 1. | Self-evaluation process is issued and completed to assess the committee’s performance. |
Executive Officer – Council and Committees of Council Governance & Strategy Committee |
An annual on-line self-evaluation form is made available around the end of November, to all members of Council for the assessment of the committee’s performance. The Governance and Strategy Committee reviews the content of the survey each September, and forwards to Council at its October meeting for approval prior to the survey going ‘live’ around November. |
| 2. | Development of a report detailing the results of the surveys | Council Secretary |
Once all members of Council have completed the evaluation, a comprehensive report detailing the results of the individual surveys will be developed. This confidential report is provided only to the Chancellor for consideration. |
| 3. | Chancellor reviews and discusses feedback. | Chancellor | The Chancellor will meet with each Council member individually to discuss their feedback. |
| 4. | Responses are collated and tabled at Council for review and discussion | Executive Officer – Council and Committees of Council | The collated and de-identified responses are summarised into a document which is then provided to Council at its first meeting of the following year, for review and discussion. |
| 5. | Development of an Action Plan to address findings. | Chancellor | An Action Plan addressing the issues identified is developed and monitored by Council to ensure the implementation of relevant modifications. |
| Activity | Responsibility | Steps | |
| 1. | A tender is issued to conduct a review of the University’s Council. | Director, Strategy |
In the early part of the year in which an external review is to be conducted, a tender is to be issued inviting submissions from external consultants to conduct a review of the University’s Council. Council is required to review its operation and performance in accordance with the standing Council resolution CM5/05/8, the HESF, Procedure for Assessment of Council Members Performance and Universities Australia ‘Voluntary Code of Best Practice for the Governance of Australian Universities’. |
| 2. | A consultant is appointed to conduct the review | Director, Strategy | A consultant should be appointed by the end of February. |
| 3. | In consultation, an appropriate evaluation will be developed to cater for the needs and circumstance of Council. | Chancellor |
A finalised format for the evaluation should be available as soon as practicable so that the review can commence in May. The evaluation will be designed to meet the current and future requirements for the governance of the University. This includes identifying any needed skills and expertise which would contribute to effective governing. |
| 4. | Development of a report detailing the results of the surveys | Chancellor |
Once all members of Council have completed the evaluation, a comprehensive report detailing the results of the individual surveys will be developed. As the full evaluation may take place over several weeks Council will be provided with regular updates on the status of the review. |
| 5. | Report is provided for consideration at Council | Chancellor |
A final report including an Executive Summary and Recommendations to be provided for the consideration of the Governance & Strategy Committee at its July meeting. This will be forwarded to the September meeting of Council for review and discussion. |
| 6. | An Action Plan is to be developed, implemented and monitored by Council | Chancellor |
An Action Plan addressing the issues identified is developed, implemented and monitored by Council to ensure the achievement of the recommendations. This Plan should include timelines for the completion of all actions. The Action Plan should be approved at the final meeting of Council for the year. Actions should be incorporated into the Council Schedule of Business to ensure relevant actions are implemented. |
Academic Board is required to review its operation and performance in accordance with the standing Council resolution CM7/08/8, the HESF, Procedure for Assessment of Council Members Performance and Universities Australia ‘Voluntary Code of Best Practice for the Governance of Australian Universities’.
In accordance with the standing resolution, Academic Board adopted a systemic and regular reviewing of its own and that of its Standing Committees performance. Academic Board will undertake self-assessments on an annual basis and a formal review with external and internal representation every three years.
| Activity | Responsibility | Steps | |
| 1. | Development of a self-evaluation which is distributed all members of Academic Board and its Standing Committees |
Academic Board Executive Executive Officer – Academic Governance |
A brief concise self-evaluation is developed by Academic Board Executive each year to be distributed electronically / hard copy to all members of Academic Board and its Standing Committees. This self-evaluation is distributed following the second last meeting for Academic Board and each of its Standing Committees annually. Academic Governance will send reminders to Board and Committee members to ensure that all self-assessments are returned. A complete listing of the Standing Committees of Academic Board can be found on the Academic Board web site http://federation.edu.au/staff/governance/academic-board/standing-committees. |
| 2. | Members complete self-evaluation | Executive Officer – Academic Governance | Once all members of Academic Board and its Standing Committees have completed the self-evaluation, a brief report detailing the results of the assessment will be developed. |
| 3. | Academic Board Annual Report is developed | Executive Officer – Academic Governance |
The collated and de-identified responses are summarised into a document which becomes part of the Academic Board Annual Report. The results are also provided to Council at its first meeting of the following year for consideration. |
| 4. | Action Plan is developed and monitored by Academic Board | Executive Officer – Academic Governance | An Action Plan addressing any issues identified is developed and monitored by Academic Board to ensure the implementation of relevant modifications. |
| Activity | Responsibility | Steps | |
| 1. | Academic Board Executive to develop Terms of Reference for the conducting of the formal review of Academic Board. | Academic Board Executive |
These Terms of Reference must be submitted to Council for approval at the June Meeting so that the external review can commence in July. Academic Board is required to review its operation and performance in accordance with the standing Council resolution CM7/08/8, Procedure for Assessment of Council Members Performance and Universities Australia ‘Voluntary Code of Best Practice for the Governance of Australian Universities’. |
| 2. | The selection of the Review Panel will take place by Academic Board Executive, | Academic Board Executive |
Refer to the approved Terms of Reference for the Review Panel membership. One member is appointed as Chair to ensure the smooth running of the Panel. |
| 3. | Panel will conduct a comprehensive review of Academic Board and its Standing Committees. | Review Panel |
In accordance with the Terms of Reference, the Panel will conduct a comprehensive review of Academic Board and its Standing Committees. This Review will include the interviewing of members of the Board and its Standing Committees, a range of University members including the Chancellor, senior executives, academic and teaching staff and students. The Review will be conducted during July to enable the Review Report to be submitted to Council for endorsement at the August meeting. |
| 4. | Review Report is been endorsed by Council. | Executive Officer – Academic Governance | Once the Review Report has been endorsed by Council it will be forwarded to Academic Board for consideration. |
| 5. | Review and implementation of any recommendations from the Review Report and development an Action Plan. | Consultation Group |
A consultation process to be initiated with the Chancellor, the Chair of Academic Board and Deputy Vice-Chancellors to plan the implementation of any recommendations from the Review Report and develop an Action Plan. The Action Plan is to be endorsed at the December Academic Board meeting. This Plan should include timelines for the completion of all actions. |
| 6. | The Action Plan addressing any issues identified is forwarded to Council for consideration. | Chancellor |
The implementation of the Action Plan is to be managed by Academic Board and monitored by Council to ensure to ensure the achievement of the recommendations. The Action Plan will be endorsed at a meeting of Council in the following year. |
The Regulatory Point of Contact enables the University to consolidate and monitor all queries to the University’s regulatory bodies: Australian Skills Quality Authority ASQA, the Tertiary Education Quality and Standards Agency (TEQSA), the Victorian Registration and Qualifications Authority (VRQA) and the Department of Jobs, Skills, Regions and Industry (DJSIR) to one contact point within the University.
This process provides a streamlined practice where one area provides all contact and information in relation to the regulatory and funding bodies.
The benefits of this process include:
- Single point of contact within the University for all regulatory body enquiries;
- Queries that may have been submitted to a regulatory body previously by an Institute/School/Department will not be resubmitted unknowingly by another Institute/School/Department;
- Consistency in the advice provided to all staff;
- The recording of all queries to ensure they are followed up; and
- The circulating of responses to all relevant areas and staff to assist others who may have the same or similar queries.
The Regulatory Point of Contact procedure ensures the University is receiving and providing consistent advice to stakeholders and minimise the confusion with the interpretation of the relevant standards, funding contracts and legislative codes and regulations.
| Activity | Responsibility | Steps | |
| A. | Any queries regarding regulatory matters from University staff to be forwarded to Quality Assurance Services. | All staff |
|
| B. | Quality Assurance Services will forward queries via the appropriate channels to the relevant regulatory body. | Quality Assurance Services |
|
| C. | Any queries for DJSIR will be forwarded in writing from Quality Assurance Services to the Manager, Reporting and Compliance for lodging with DJSIR. | Quality Assurance Services / Manager, Reporting and Compliance |
|
| D. | Query responses received from the regulatory body will be processed by responding to the University staff member initiating the query. | Quality Assurance Services |
|
- The Dean, Quality, Partnerships and Accreditation (as the Approval Authority) is responsible for monitoring the implementation, outcomes and scheduled review of this framework.
- The Manager, Strategic Regulatory Services (as the Document Owner) is responsible for maintaining the content of this framework as delegated by the Approval Authority.
The Quality Framework will be communicated throughout the University via:
- An Announcement Notice via FedNews website and on the 'Recently Approved Documents' page on the 'Policies, Procedures and Forms @ the University' website to alert the university-wide community of the approved Policy.
The Quality Framework will be implemented throughout the University through the following mechanism:
- An Announcement Notice via FedNews website and on the 'Recently Approved Documents' page on the 'Policies, Procedures and Forms @ the University' website to alert the University-wide community of the approved Policy.
 Prev
Prev Up
Up Next
Next